Wisdom tooth surgery
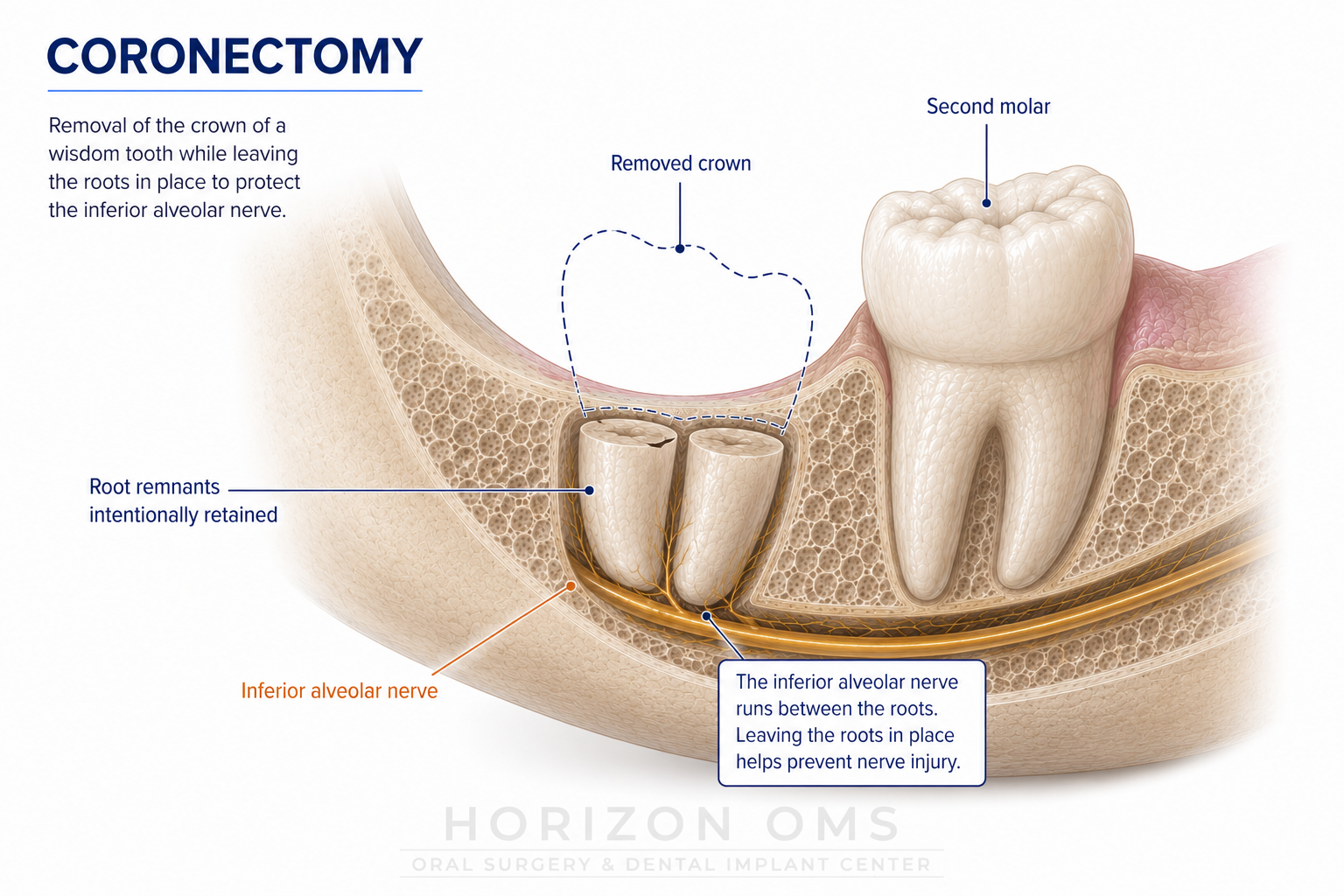
Coronectomy
A nerve-sparing option for selected lower wisdom teeth whose roots are very close to the inferior alveolar nerve.
What is a coronectomy?
A coronectomy is a planned alternative to complete wisdom tooth removal for certain lower wisdom teeth. The crown—the part of the tooth that can create infection, inflammation, or damage to the neighboring molar—is removed while healthy, stable roots are intentionally left in place.
The purpose is to avoid unnecessary disturbance of the inferior alveolar nerve, which provides feeling to the lower lip and chin. Coronectomy is considered only when the tooth needs treatment and imaging shows that complete root removal may carry an increased nerve risk.
At Horizon OMS in Lombard, Illinois, the recommendation is based on the tooth’s condition, the nerve relationship seen on imaging, and whether retaining the roots offers a better balance of treatment benefit and risk.
Why the nerve relationship matters
The inferior alveolar nerve runs through the lower jaw, sometimes immediately beside or between wisdom tooth roots. Most wisdom teeth can be removed completely without lasting nerve problems. In a smaller group of patients, however, the roots and nerve are so closely related that removing the roots may increase the chance of temporary or, rarely, persistent numbness.
A panoramic X-ray often identifies warning signs. A CBCT scan may be recommended when a three-dimensional view could clarify the relationship or change the treatment plan.
When may a coronectomy be considered?
- A lower wisdom tooth has a reason for treatment, such as recurrent inflammation, decay, or risk to the second molar.
- The roots appear to be in very close contact with the inferior alveolar nerve.
- The retained roots are healthy and stable enough to remain in place.
- The patient can return for follow-up if needed.
Coronectomy may not be appropriate when infection or disease involves the roots, when the roots are already mobile, or when a cyst or other condition requires the entire tooth to be removed. Sometimes the safest plan can only be finalized during surgery if a root becomes loose.
What does the procedure involve?
The crown of the wisdom tooth is carefully separated and removed while the roots are left undisturbed. The area is then cleaned and closed so bone and gum tissue can heal over the retained roots. The procedure may be completed with local anesthesia or IV sedation, depending on the case and patient preference.
In selected cases, platelet-rich fibrin (PRF) may be used as an adjunct to support early healing.
Benefits and the main tradeoff
The intended benefit is a lower risk of inferior alveolar nerve injury compared with complete extraction in carefully selected high-risk teeth. Randomized trials and systematic reviews generally support coronectomy as a useful nerve-sparing option when the roots are suitable to retain.1, 2
What happens to the retained roots?
Some retained roots move as healing occurs. In many cases, they move away from the nerve. This movement alone does not mean there is a problem and does not automatically require treatment.
If a root later becomes exposed, painful, or infected, it may need to be removed. When removal is necessary, the root may be farther from the nerve than it was at the original surgery.
Risks and follow-up
Short-term recovery is generally similar to other lower wisdom tooth procedures and may include swelling, soreness, bruising, bleeding, jaw stiffness, infection, or dry socket. Nerve disturbance remains possible even though reducing that risk is the reason coronectomy is considered.
The procedure-specific concern is the possibility of later treatment for a retained root. Follow-up is individualized; an X-ray finding by itself does not always require another procedure.
Why oral and maxillofacial surgery evaluation matters
The key decision is not simply whether the roots look close to the nerve. It is whether the tooth should be observed, removed completely, or treated with coronectomy. Oral and maxillofacial surgeons routinely evaluate impacted wisdom teeth, jaw-nerve anatomy, and three-dimensional imaging, and can adjust the plan when surgical findings differ from the X-ray appearance.
For referring dentists, a recent panoramic image and information about symptoms, prior infection, periodontal findings, and the condition of the adjacent second molar are helpful. The goal is collaborative planning around the option that offers the best balance of treatment benefit and risk.
Recovery
Swelling and soreness are usually most noticeable during the first several days and then gradually improve. Patients receive individualized instructions for diet, oral hygiene, medications, and activity. General guidance is available in our wisdom teeth aftercare resource.
Contact the office for worsening pain after initial improvement, fever, drainage, increasing swelling, uncontrolled bleeding, new or worsening numbness, or a hard structure becoming exposed through the gum.
- Di Spirito F, et al. Re-Intervention Rate, Timing, and Indications Following Coronectomy of Mandibular Third Molars: A Systematic Review of Systematic Reviews. Journal of Clinical Medicine. 2025. Full text
- Cervera-Espert J, et al. Coronectomy of impacted mandibular third molars: A meta-analysis and systematic review of the literature. Med Oral Patol Oral Cir Bucal. 2016. Full text
- American Association of Oral and Maxillofacial Surgeons. Management of Third Molar Teeth. Clinical guidance