Procedures
Bone Grafting
Research-based socket preservation, ridge augmentation, and grafting to preserve bone volume for predictable dental implant planning.
Why bone grafting matters after an extraction
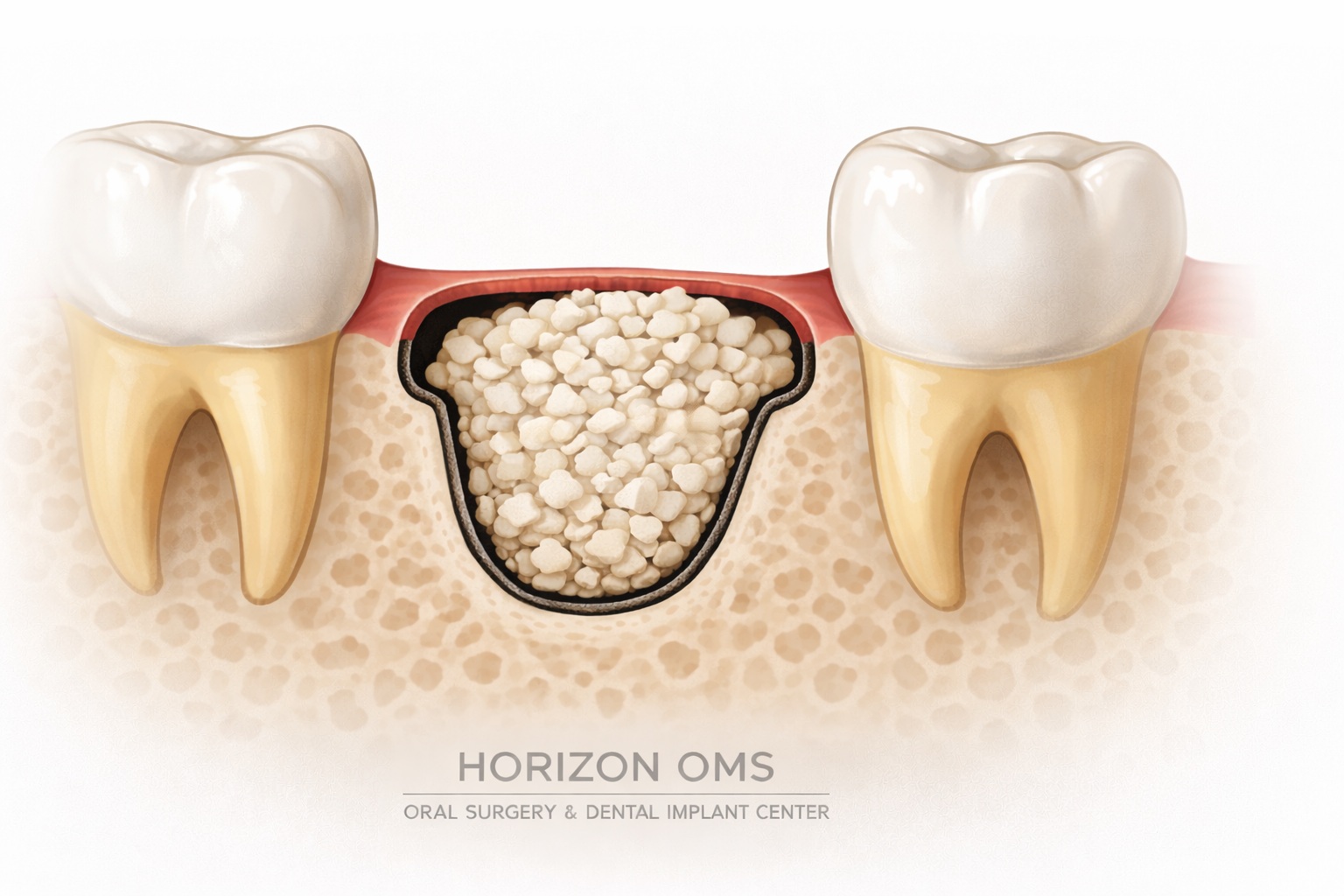
When a tooth is removed, the surrounding jawbone begins to remodel. The outer, cheek-side wall of the socket—called the buccal plate—is often thin and is the part most likely to shrink inward. That early collapse can make a future dental implant harder to place in the ideal position, especially in the front of the mouth and in the upper back jaw near the sinus.
Socket preservation or ridge preservation means placing graft material into the extraction site at the same visit. The goal is not to “overbuild” the area. The goal is to preserve as much natural ridge width and height as possible while the body heals.
How the graft becomes your own bone
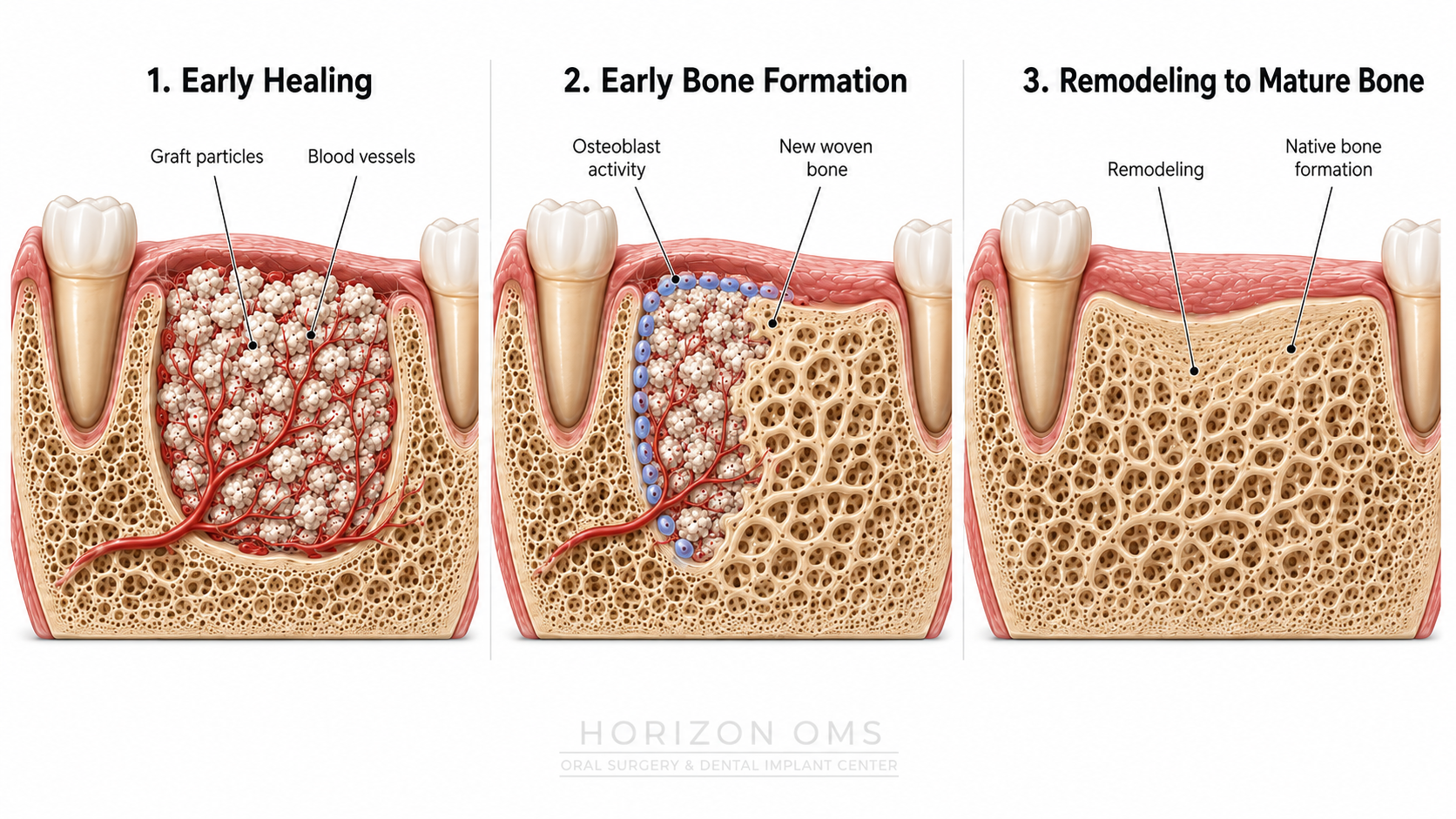
Bone graft material acts as a biologic scaffold. Blood vessels, healing cells, and bone-forming cells migrate through the graft as the socket heals. Over time, the site remodels: the initial clot becomes early woven bone, then stronger mature bone. Depending on the material used, some slowly resorbing graft particles may remain for a long period, but the clinical goal is a stable, well-vascularized ridge that can support a future implant.
When appropriate, we may combine grafting with platelet-rich fibrin (PRF), which is made from a small sample of your own blood. PRF forms a natural fibrin matrix that can help stabilize the clot, support soft-tissue healing, and deliver growth factors during the early healing period.
Common situations we treat
- Ridge preservation at the time of extraction to reduce socket collapse and maintain contour
- Socket grafting when a future dental implant is planned
- Buccal plate defects where infection, fracture, or a difficult extraction has weakened the outer wall
- Ridge augmentation to widen or rebuild areas that are already too thin for ideal implant placement
- Posterior upper-jaw grafting to preserve bone height near the sinus and potentially reduce the need for a future Sinus Lift
- Site development before implants when bone volume, width, or position is not adequate
Can socket grafting help avoid a sinus lift?
Sometimes, yes. After upper molars are removed, the maxillary sinus can expand downward while the ridge resorbs upward. This can leave less vertical bone for an implant. In selected posterior maxillary sites, ridge preservation can help maintain ridge height and may reduce the chance of needing a larger lateral-window sinus lift later. It may allow a smaller internal sinus lift—or, in some cases, no sinus lift at all.
That said, it is not a guarantee. The decision depends on your starting bone height, sinus anatomy, infection history, implant plan, and the timing of treatment. A CBCT scan lets us measure this accurately instead of guessing from a two-dimensional X-ray.
What to expect during treatment
Your evaluation may include a CBCT scan to measure ridge width, height, sinus position, and nearby anatomy. The grafting approach is customized to the defect: a simple socket graft is very different from a wider ridge augmentation or staged implant site development.
Many grafting procedures are performed comfortably with office-based IV sedation, especially when grafting is combined with extractions or implant planning. Smaller grafts may also be done with local anesthesia when appropriate.

Healing & timing before implants
Smaller socket preservation grafts often heal faster than larger ridge augmentations, but the site still needs time to consolidate before implant placement. The timeline depends on the tooth location, defect size, graft type, soft-tissue closure, medical history, and whether infection was present.
During early healing, the priority is protecting the clot and graft. We typically recommend a soft diet, careful hygiene, and avoiding pressure on the grafted area. If a temporary prosthesis is used, it may need to be adjusted so it does not compress the healing site.
Research-based notes
- Systematic reviews show that extraction sites naturally lose ridge width and height, with horizontal/buccal changes often being the most clinically important for implant placement.
- Alveolar ridge preservation has been shown to reduce physiologic ridge shrinkage compared with extraction alone.
- Recent posterior maxilla studies suggest ridge preservation can reduce sinus pneumatization and reduce the need for additional sinus floor augmentation at implant placement.
- PRF research suggests the greatest benefit is often during early soft-tissue and socket healing, especially in the first few months.
Selected literature: Avila-Ortiz et al., 2019; Mahardawi et al., 2025; Khoury et al., 2024; Alrayyes et al., 2022; Al-Maawi et al., 2021.