Procedures
Corrective Jaw Surgery
Surgical correction of jaw alignment to improve function, stability, and facial balance. Also known as orthognathic surgery.

What is orthognathic surgery?
Orthognathic surgery is corrective jaw surgery used to reposition the upper jaw, lower jaw, or chin when the jaw relationship cannot be corrected predictably with orthodontics alone. The goal is not just to “straighten the bite” — it is to build a stable bite, improve jaw function, support facial balance, and address airway or TMJ considerations when they are part of the larger diagnosis.
Most patients are treated in close coordination with an orthodontist. Orthodontic treatment aligns the teeth so the jaw movements can be planned accurately, and the surgical plan is usually built from CBCT imaging, bite records, facial analysis, and digital simulation.
Corrective jaw surgery may involve one or more areas:
- Maxillary surgery — upper jaw surgery, most commonly a Le Fort I osteotomy.
- Mandibular surgery — lower jaw surgery, most commonly a bilateral sagittal split osteotomy (BSSO).
- Genioplasty — chin surgery that can improve facial balance and, in select airway cases, help advance tongue-supporting muscles.
Single-jaw vs. double-jaw surgery
Orthognathic surgery can be performed on the upper jaw (maxilla), the lower jaw (mandible), or both jaws depending on the bite relationship, facial balance, and airway or functional goals.
- Single-jaw surgery may be recommended when correcting one jaw provides a stable bite and balanced result.
- Double-jaw surgery is considered when both jaws contribute to the discrepancy or when the most stable, predictable correction requires coordinated upper and lower jaw movements.
- Chin surgery (genioplasty) may be added when the chin position needs to be refined independently from the bite.
Common indications
- Difficulty chewing, biting, or bringing the teeth together comfortably
- Underbite, overbite, crossbite, open bite, or severe malocclusion
- Jaw asymmetry, facial imbalance, or occlusal cant
- Speech, swallowing, or lip-closure difficulty related to jaw position
- Obstructive sleep-related breathing issues in select patients
- Jaw discrepancies associated with TMJ disease or prior facial trauma

Treatment planning
Successful orthognathic surgery requires close coordination between the oral surgeon and orthodontist. Planning often includes digital imaging, dental models or scans, bite registration, facial photographs, and simulation to guide precise surgical movements. In select cases, corrective jaw surgery may also be coordinated with TMJ joint procedures when indicated.
3D Virtual Surgical Planning (VSP)
When appropriate, we use 3D Virtual Surgical Planning (VSP) — a digital workflow that combines CBCT (3D CT) imaging, digital dental records, and computer simulation to plan the surgery before the operation. VSP allows us to preview jaw movements, help design surgical splints/guides, and translate the plan more precisely in the operating room. Reviews of VSP in orthognathic surgery report improved predictability and accurate transfer of the treatment plan compared with traditional methods.1, 2
If your case involves complex asymmetry, airway considerations, a multi-piece Le Fort I, or combined TMJ procedures, VSP can be especially helpful for coordinating jaw position, bite fit, and facial balance.
Types of corrective jaw surgeries
The exact surgical plan is customized to the bite, airway, facial balance, and orthodontic setup. Some patients need one jaw moved, while others benefit from coordinated upper jaw, lower jaw, and/or chin movements.
Upper jaw surgery: Le Fort I maxillary osteotomy
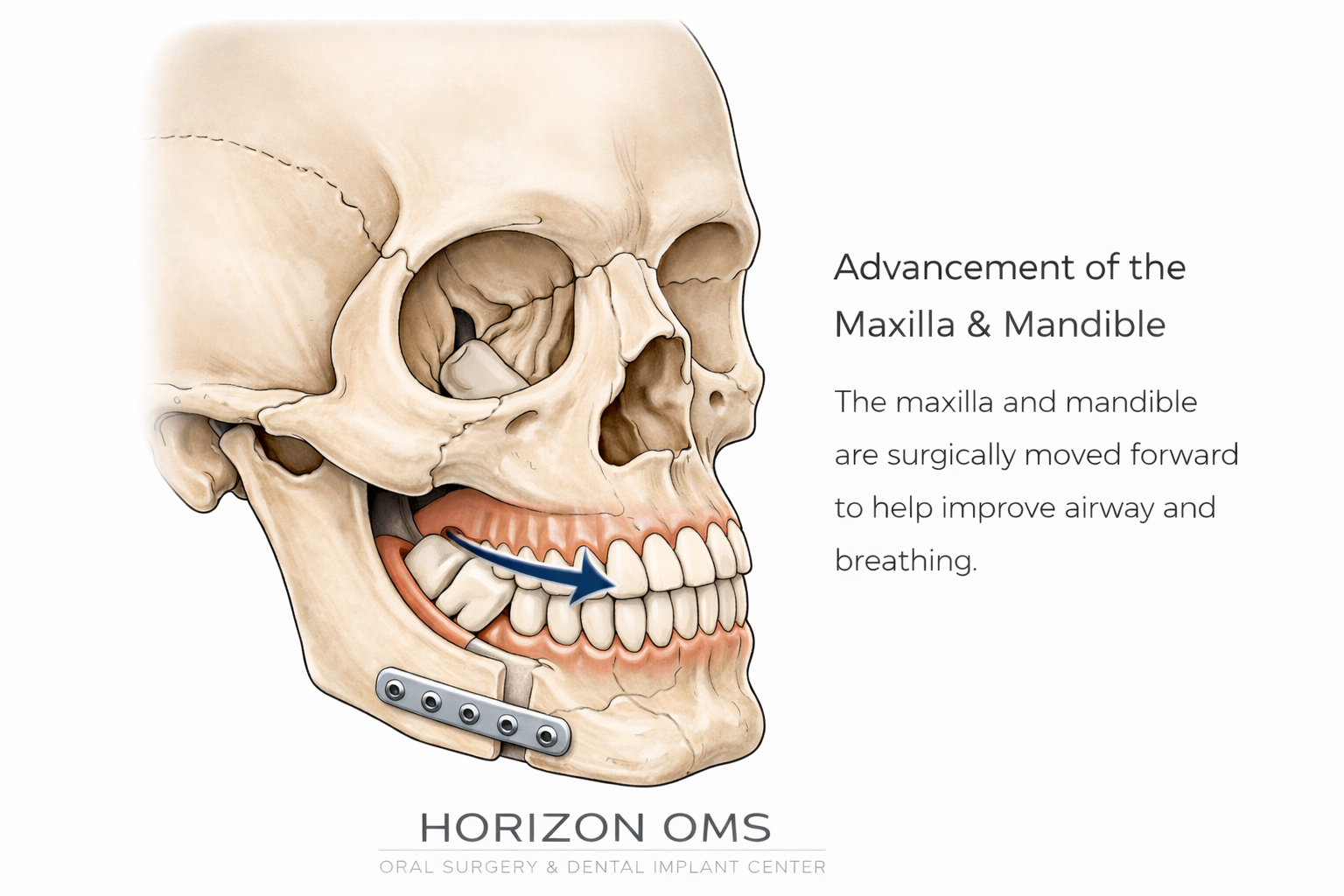
Maxillary surgery is used to reposition the upper jaw when the maxilla is too far back, too far forward, vertically excessive, vertically deficient, tilted, narrow, or contributing to an open bite or facial asymmetry. The most common approach is a Le Fort I osteotomy.
Incision design: all intraoral
The incision is made inside the mouth, typically in the upper gumline/vestibule above the teeth. There is no external facial incision for a routine Le Fort I osteotomy. Once the upper jaw is accessed, the bone cuts are planned to mobilize the maxilla while protecting the teeth, roots, nasal floor, sinuses, and surrounding soft tissue.
What movements can be planned?
- Advancement to bring a retrusive upper jaw forward.
- Impaction to move the upper jaw upward, often used for vertical maxillary excess or excessive gum display.
- Downgrafting or vertical repositioning in select cases where additional vertical support is needed.
- Yaw, roll, and pitch correction to correct canting, asymmetry, or three-dimensional imbalance.
Single-piece vs. multi-piece Le Fort I
A single-piece Le Fort I moves the upper jaw as one unit and is often used when the arch width and tooth-level relationships are already well coordinated orthodontically. A multi-piece Le Fort I divides the maxilla into two or more segments, allowing the surgeon and orthodontist to address transverse width problems, arch-form issues, open bite patterns, or tooth-bearing segment discrepancies that cannot be corrected as well by moving the upper jaw as one block.
Multi-piece movements require careful planning because tooth roots, gum tissue, palatal blood supply, and segment stability all matter. This is one reason digital planning and orthodontic coordination are so important.
Lower jaw surgery: BSSO mandibular osteotomy
Lower jaw surgery most commonly uses a bilateral sagittal split osteotomy, or BSSO. This technique allows the tooth-bearing portion of the lower jaw to be advanced, set back, rotated, or leveled while keeping broad bone contact for healing.
How the surgery is carried out around the IAN
The inferior alveolar nerve (IAN) runs inside the mandible and supplies sensation to the lower lip, chin, and lower teeth. During planning, CBCT imaging helps evaluate the nerve canal and the thickness and shape of the lower jaw. During surgery, the bone cuts are designed to create a controlled split while keeping the nerve protected within the bony segment whenever possible. If the nerve is visualized during the split, it is handled carefully and protected while the jaw is positioned and stabilized.
Temporary numbness or altered sensation is still possible because the nerve is close to the surgical field. The goal is to reduce risk through imaging, controlled osteotomy design, careful splitting technique, and precise fixation.
Incisions and cheek access
The main incisions for BSSO are inside the mouth. In some cases, a very small cheek access point is used for instrumentation or screw placement. This is typically tiny and heals very cosmetically — often far smaller than an acne scar.
TMJ coordination
For patients with significant jaw-joint disease, degenerative joint changes, or prior TMJ surgery, corrective jaw surgery may sometimes be coordinated with TMJ procedures. Learn more about joint-focused care on our TMJ Disorders and TMJ Surgery page.
Chin surgery: genioplasty
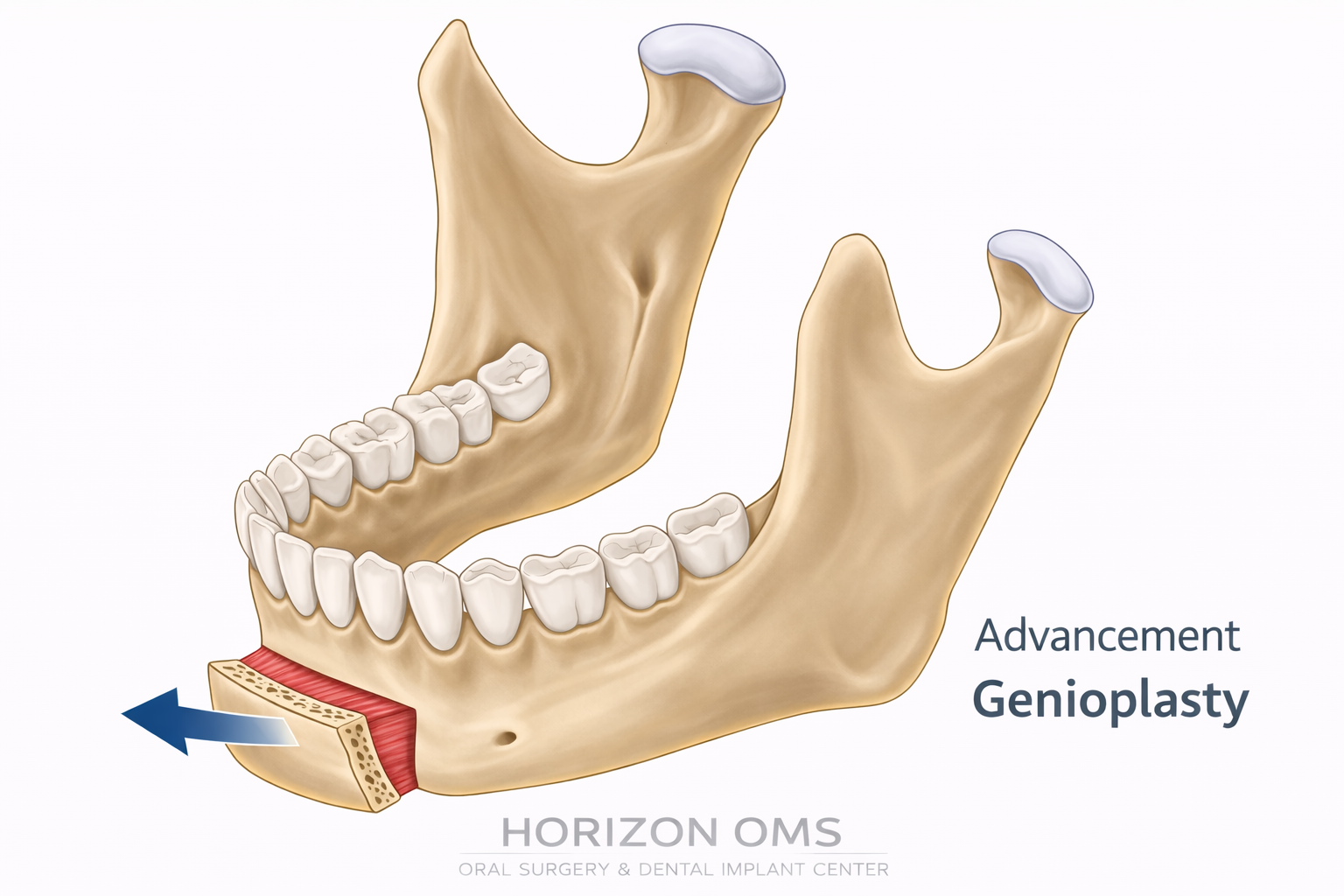
Genioplasty changes the position or shape of the chin without changing how the teeth fit together. It can be performed by itself or combined with upper jaw surgery, lower jaw surgery, or double-jaw surgery when the chin position needs to be adjusted independently from the bite.
Common types of genioplasty
- Sliding advancement genioplasty moves the chin bone forward to improve projection and lower-face balance.
- Vertical genioplasty can lengthen or shorten the lower face when vertical chin height is part of the concern.
- Asymmetry correction can shift or reshape the chin to improve midline and lower-face balance.
- Reduction or setback genioplasty may be used when the chin is overly prominent relative to the rest of the face.
High genioplasty and airway-focused chin surgery
In select patients, a higher or specially designed genioplasty can advance the genial tubercle region where the genioglossus muscles attach. These muscles help support the tongue base, so advancing this area can be part of an airway-focused plan. When the primary goal is airway improvement, this may be discussed alongside maxillomandibular advancement (MMA) and sleep apnea surgery.
Not every chin procedure is an airway procedure. The design depends on whether the goal is facial balance, lip competence, airway support, or a combination of factors.
Surgery & recovery
Procedures are typically performed in a hospital setting under general anesthesia. Many patients stay overnight for monitoring, then continue recovery at home with a staged return to normal activity. Recovery involves a period of swelling, dietary modification, oral hygiene changes, and close follow-up with your surgical and orthodontic teams.
Modern jaw surgery usually uses small plates and screws to stabilize the new jaw position. Many patients are not “wired shut” in the old-fashioned sense, although orthodontic elastics are commonly used to guide the bite while the jaws heal.
Cases from Our Practice




This patient underwent a LeFort I advancement and rotation, bilateral sagittal split osteotomies (BSSO), and genioplasty to correct facial imbalances, improve upper jaw, lower jaw, and chin harmony, and improve her airway and breathing.
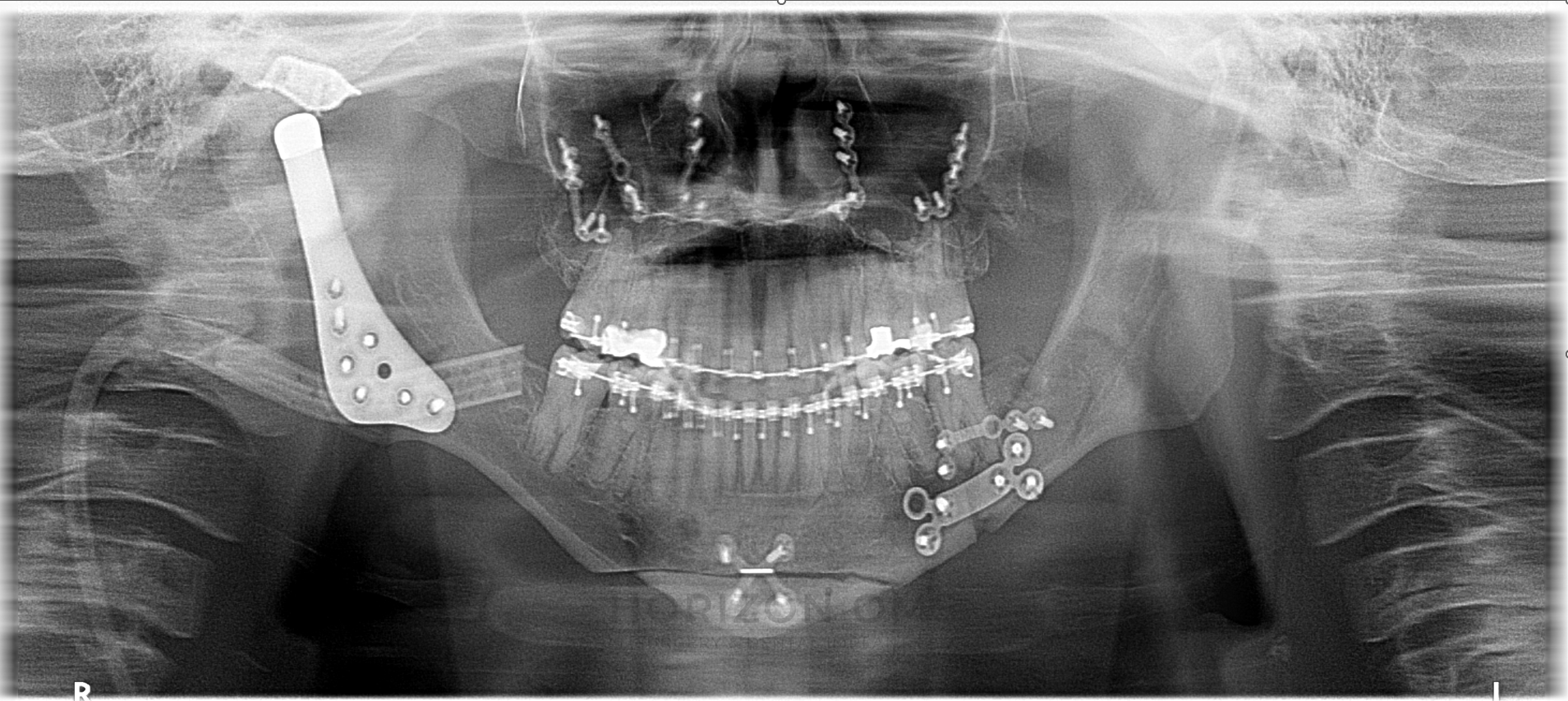
This patient presented with TMJ pain, limited mouth opening, jaw and chin deviation, and restless sleep related to airway collapse. Treatment involved bilateral TMJ replacement with simultaneous Le Fort I advancement to restore lower facial height, address the collapsed airway and compensatory maxillary changes, and genioplasty to improve chin asymmetry and facial profile. At follow-up, she was incredibly happy with the result and reported resolution of pain with significantly better sleep.
This patient underwent double-jaw corrective surgery with maxillary advancement and mandibular setback. Temporary anchorage devices (TADs) were placed in the maxilla to give the orthodontic team precise anchorage for closing and redistributing spaces after surgery. A stable, well-finished result depends on close coordination between the surgeon and orthodontist before surgery, throughout planning, and during postoperative orthodontic finishing.
This case combined Le Fort I advancement, left sagittal split osteotomy, and right custom total joint replacement to restore facial balance, improve TMJ function, and address jaw-joint pain. Learn more about TMJ surgery and jaw-joint care.
This case shows a Le Fort I maxillary advancement coordinated with clear-aligner orthodontic treatment. Not every corrective jaw surgery case requires traditional braces; some patients can be prepared with Invisalign or other clear-aligner systems when the tooth movements, bite setup, and surgical plan are closely coordinated with the orthodontist.
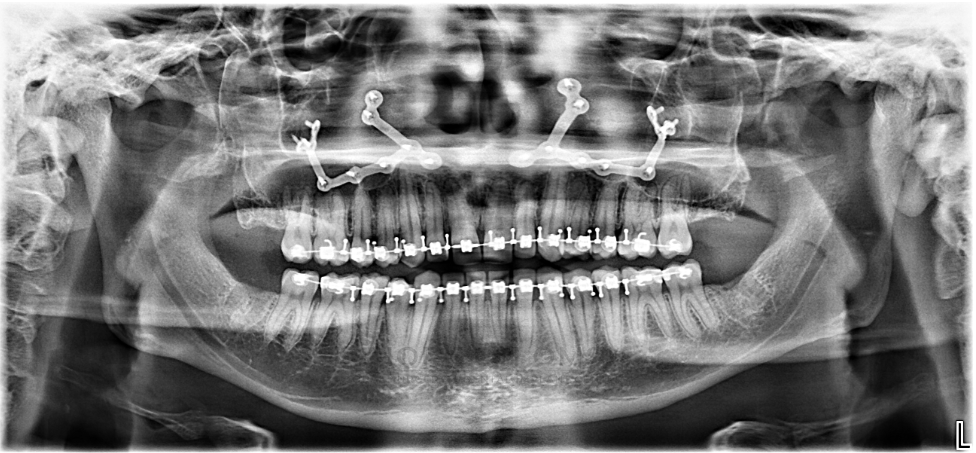
This case shows a Le Fort I maxillary advancement coordinated with traditional orthodontic brackets. Braces remain a very effective way to align the teeth before and after jaw surgery, especially when precise bite control and surgical orthodontic finishing are needed.
Cases personally treated by Dr. Ali Al-Qudsi, board-certified oral and maxillofacial surgeon. Individual anatomy, healing, and results vary.
- Shalabi MM, et al. Accuracy of 3D Virtual Surgical Planning Compared to Traditional Planning. 2024 (review). Full text
- Alkaabi S, et al. Virtual and traditional surgical planning in orthognathic surgery. 2022 (systematic review/meta-analysis). Abstract
- American Association of Oral and Maxillofacial Surgeons. Indications for Orthognathic Surgery. Clinical paper