Procedures
Tori Removal
Tori are benign bony growths that can become a real problem when they rub, trap food, block dentures or appliances, or complicate dental treatment.
What are tori?
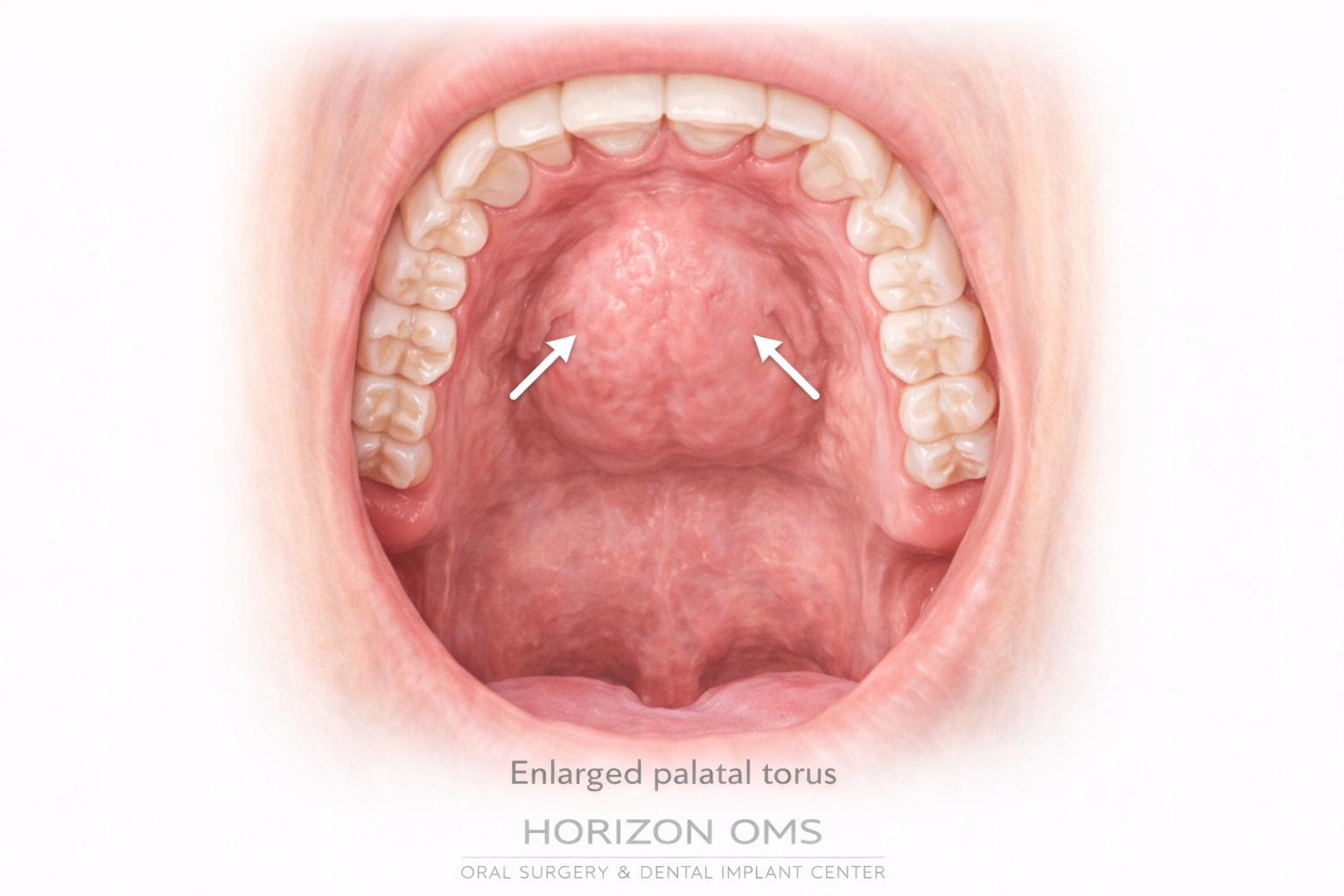
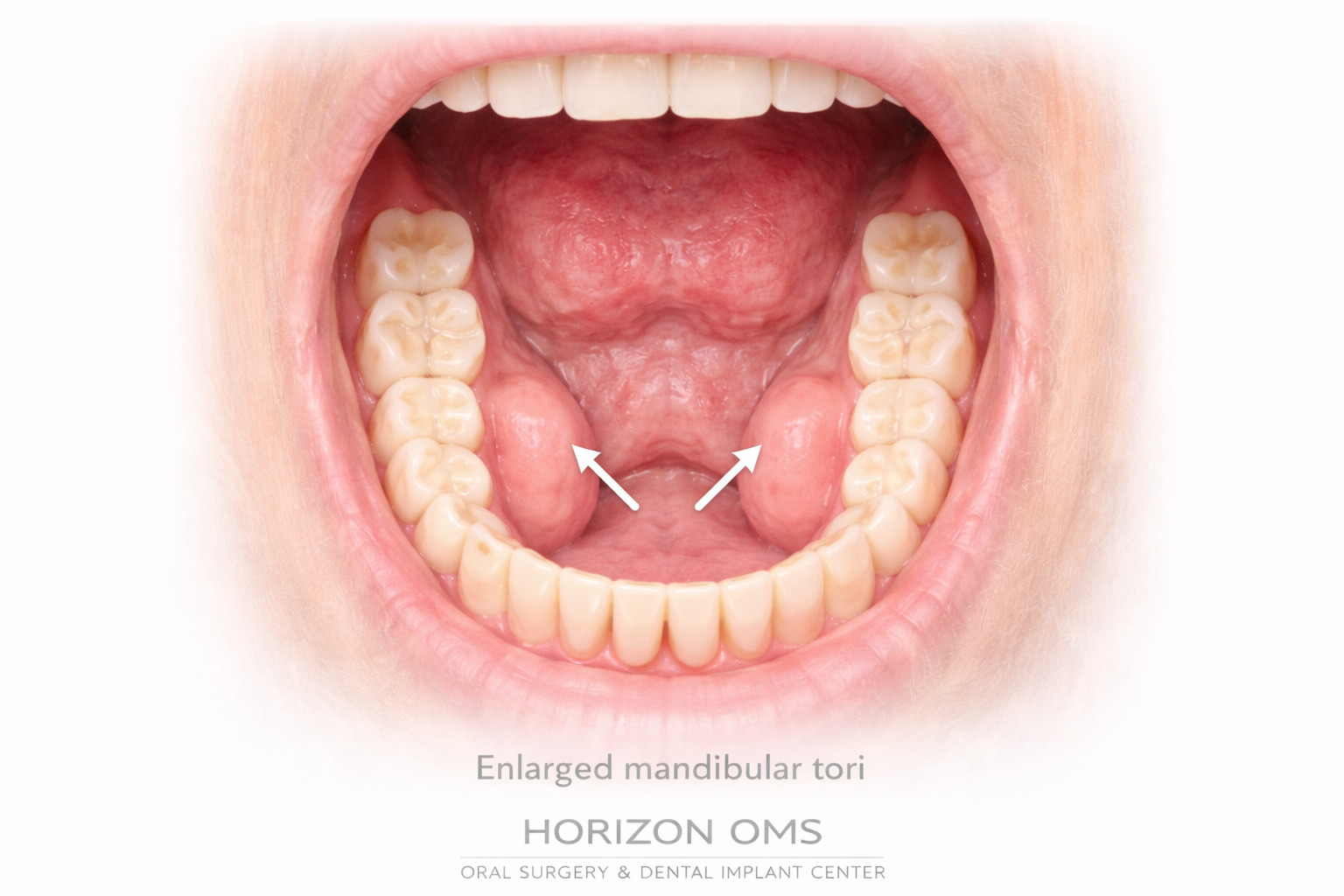
Tori are benign overgrowths of dense cortical bone. They most commonly appear along the middle of the hard palate (palatal torus) or on the tongue-side of the lower jaw near the premolars (mandibular tori). They are not cancer, and many patients never need them removed.
The issue is usually practical: the gum tissue over a torus can be thin, the area can ulcerate when it rubs against food or a dental appliance, and large tori can limit tongue space, hygiene access, denture fit, impressions, or future restorative treatment.
Why do tori happen?
Tori are usually multifactorial. Research supports a combination of inherited tendency, individual bone biology, and local mechanical forces. In plain English: some people are built more likely to form them, and heavy bite forces may help stimulate or maintain that extra bone.
That is why tori are often discussed in the same conversation as TMJ symptoms, clenching, grinding, worn teeth, masseter enlargement, and jaw muscle fatigue. Not every patient with tori is a grinder, and not every grinder develops tori, but the overlap matters when planning long-term care.
When observation is enough
Small, smooth, asymptomatic tori can usually be monitored during routine dental visits. If they are stable, easy to clean around, and not interfering with treatment, leaving them alone is often the best decision.
Reasons tori may need removal
- Denture or appliance interference: tori may prevent a denture, partial, sleep appliance, orthodontic appliance, or surgical guide from seating properly.
- Repeated sores or ulceration: the tissue over tori is often thin and can break down from chips, crusty foods, toothbrush trauma, or appliance pressure.
- Speech, chewing, or tongue-space issues: larger mandibular tori can crowd the tongue and make chewing or speaking feel awkward.
- Hygiene problems: food and plaque may collect around irregular bony contours, especially when access is limited.
- Planned dental work: removal may be needed before dentures, restorative reconstruction, impressions, grafting, or other procedures where the tori block access or create instability.
- Diagnostic concern: most tori are easy to recognize clinically, but any one-sided, painful, ulcerated, numb, or rapidly changing bony swelling deserves careful evaluation.
How tori removal is planned
Planning depends on the location, size, shape, gum thickness, and the reason for removal. For mandibular tori, we pay close attention to the floor of mouth, tongue-side tissue, and nearby anatomy. For palatal tori, we consider the thin palatal tissue and the need for smooth contouring if a denture or appliance is planned.
Imaging may be used when the anatomy is large, asymmetric, or part of a broader treatment plan. If the removal is being done for denture or appliance fabrication, timing is coordinated so the tissue has enough time to heal before the final prosthesis is made.
How tori removal works
Tori removal is performed with local anesthesia, with IV sedation available when appropriate for comfort. The gum tissue is carefully opened, the excess bone is reduced in a controlled way, the surface is smoothed, and the tissue is closed with sutures.
The goal is not just to “take off the bump.” The goal is to create a smooth, maintainable contour that heals well and supports the reason the procedure was recommended in the first place—comfort, hygiene, appliance fit, denture fit, or restorative access.
Recovery & aftercare
Swelling, soreness, and tightness are expected for several days. A soft diet is usually recommended at first, especially because hard or sharp foods can traumatize the thin tissue as it heals. We provide written after-surgery instructions and review diet, rinsing, medication use, and activity restrictions.
Initial gum healing often takes 1–2 weeks, but the area continues to settle and remodel over the following weeks. If dentures, partials, retainers, or other appliances are involved, they may need to be adjusted or delayed until the tissue is ready.
Can tori come back?
Recurrence is not the usual expectation, but it is possible. Published case reports show that some mandibular tori can recur after surgical removal, including long-term recurrence over many years and rare early recurrence. That is why the consultation should include the “why” behind the tori—not just the mechanics of removing them.
For heavy clenchers or grinders, managing jaw muscle overload may be part of the long-term plan. That may include appliance therapy through your dentist, TMJ-focused care, habit modification, and in select patients Botox for TMJ / masseter overactivity. Botox does not directly remove tori and cannot guarantee they will not regrow, but reducing excessive masseter activity may help with clenching-related pain, muscle fatigue, and high bite-force patterns in appropriate patients.
Research notes
Tori are described in the literature as common, benign oral exostoses with multifactorial causes, including hereditary and environmental/mechanical factors. Studies have also reported associations between mandibular tori and parafunctional activity or TMJ-related findings. Recurrence after removal appears uncommon but has been documented in case reports, including long-term follow-up cases.
- García-García et al. Current status of the torus palatinus and torus mandibularis.
- Morrison & Tamimi. Oral tori are associated with local mechanical and systemic factors.
- Sirirungrojying & Kerdpon. Relationship between oral tori and temporomandibular disorders.
- Brunsvold et al. Recurrence of mandibular tori after surgical removal.
- Valentin et al. Early recurrence of mandibular torus following surgical resection.